music_note
videocam
×
Close
search
Sign Up
Login
Member Login
Remember me
Forgot password?
Sign Up
Videos
Home
Groups
AI
Live News
Stores
People
Blogs
Topics
Photos
Events
Videos
×
Close
More from this channel
Family's fury as hospital unit where father died after 'wrong person' surgery mix-up investigated
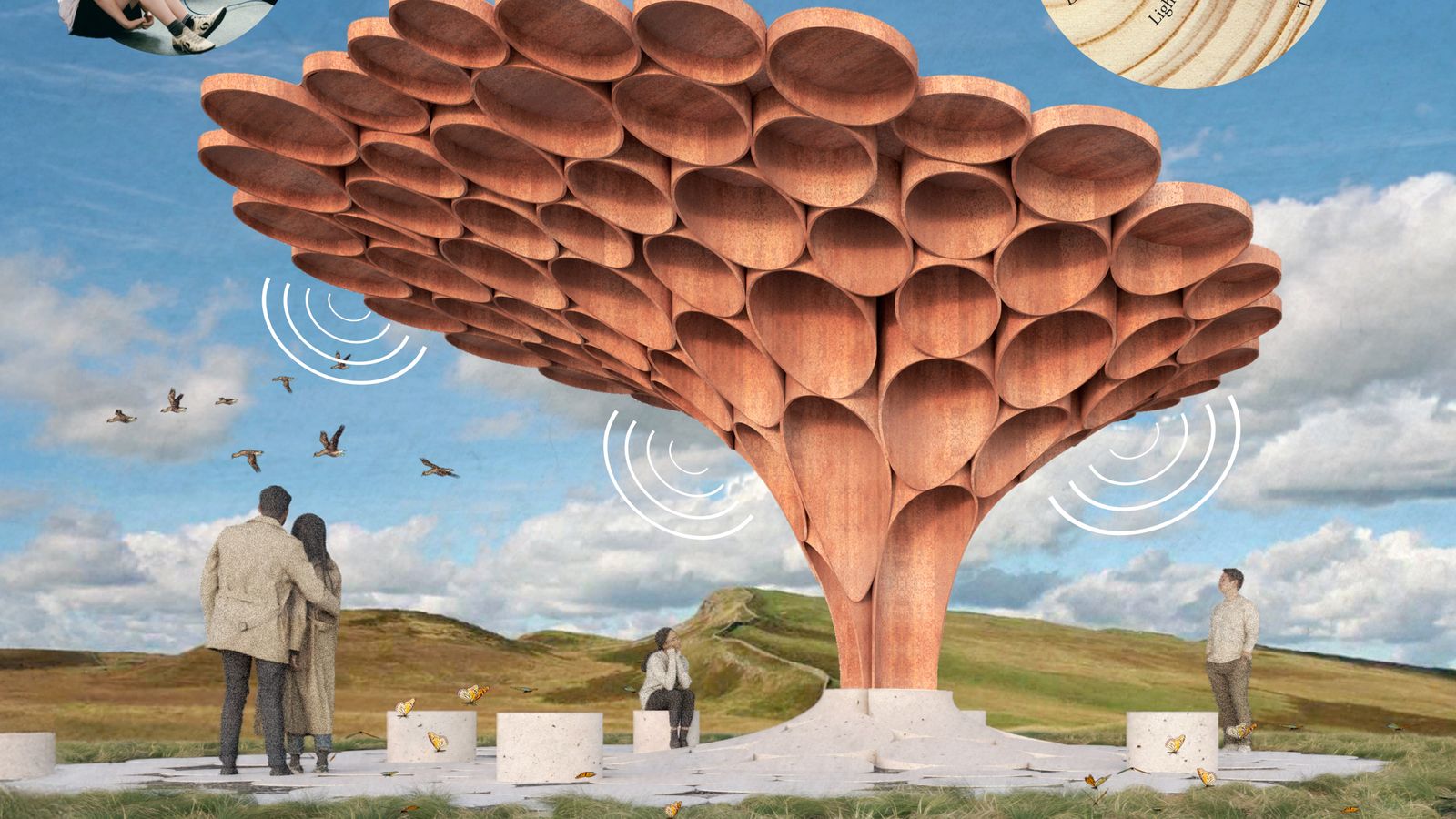
What future do you want for Sycamore Gap tree?
Ex-Labour minister who was confronted by Joanna Lumley in TV showdown has died
Book claiming Meghan 'brainwashed' Harry is 'deranged conspiracy', says his spokesperson
Man found dead in wheelie bin
Girl, 15, killed in three-vehicle motorbike crash with boy arrested
Woman arrested on suspicion of murder after baby dies in fall 'from a height' in central London
Uninsured driver jailed for killing 'cheerful' four-year-old girl
Family's anger as hospital unit where father died after surgery mix-up investigated
Driver who partied after killing teenage friends in crash sentenced
Woman who was paid £20k after being told she had scooped Paddy Power's £1m jackpot wins court case
View Original Article
thumb_up
0
thumb_down
0
share
Share
0
people liked this
Comments (
0
)
Modal title
×
Modal title
AI Article
close
Send
×
Share










Comments (0)